The Comprehensive Guide to Dental Implants: Biology, Technology, and Clinical Realities
The field of restorative dentistry has undergone a radical transformation over the past several decades. For generations, individuals suffering from tooth loss were limited to superficial surface-level prosthetics like removable dentures or fixed dental bridges. While these traditional modalities offered basic cosmetic concealment, they frequently failed to stop long-term biological deterioration and presented significant functional limitations.
https://www.tidental.com.m...
Today, dental implants represent the undisputed gold standard for tooth replacement in modern clinical practice. By serving as biocompatible, structural anchors that integrate directly with the human facial skeleton, implants closely match the biological efficiency, tactile sensation, and functional bite force of natural dentition.
For patients managing single-tooth gaps due to trauma, multiple missing segments from progressive decay, or complete edentulism (total tooth loss), dental implants provide a reliable, predictable option for comprehensive oral rehabilitation. This comprehensive clinical article covers the structural engineering, biological mechanisms, diagnostic protocols, and contemporary workflows defining modern dental implantology.
Anatomy and Structural Engineering of an Implant System
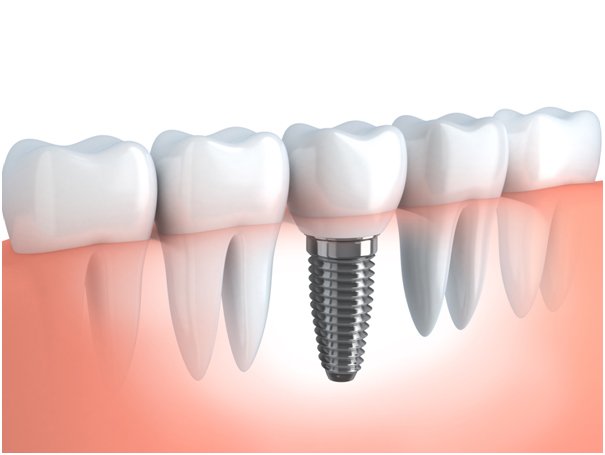
A dental implant is not a singular prosthetic component, but rather an assembly of micro-engineered parts that function as a unified structural system. The long-term success of an implant relies on the mechanical connections between three key elements:
The Implant Fixture (Post): This is the screw-like cylinder that is surgically inserted deep into the cortical and cancellous bone of the maxilla (upper jaw) or mandible (lower jaw). It acts as an artificial root. Modern fixtures are heavily engineered using bio-inert materials—most commonly grade 4 or grade 5 titanium alloys, or highly resilient zirconia ceramics. The surface texture is often modified via sandblasting, large-grit acid-etching, or hydrophilic coatings to maximize surface area and accelerate initial cellular attachment.
The Abutment: This is a precision-machined intermediate connector piece that attaches directly into the internal chamber of the implant fixture via an internal hex or conical connection. The abutment transitions the implant system from an intraosseous (inside the bone) anchor to a transmucosal (through the gum tissue) platform, serving as the solid core onto which the visible prosthesis is anchored.
The Prosthetic Restoration: The definitive aesthetic and functional component of the system. Depending on the patient's structural needs, this may consist of a single custom crown, a multi-unit fixed bridge, or a full-arch overdenture. These are typically fabricated from advanced ceramics, lithium disilicate, or monolithic zirconia blocks using computer-aided manufacturing to match natural teeth.
The Biology of Osseointegration
The scientific foundation of modern implantology relies on the biological phenomenon of osseointegration. Discovered by Swedish orthopedic surgeon Dr. Per-Ingvar Brånemark, osseointegration is defined as the direct, rigid structural and functional connection between living bone tissue and the surface of a load-bearing artificial implant, without any intervening soft tissue layers.
When a titanium or zirconia fixture is surgically advanced into a prepared osteotomy (bone site), it achieves immediate mechanical stability known as primary stability. This initial mechanical lock depends entirely on the physical threads of the screw compressing the surrounding bone.
Following placement, a complex cascade of cellular wound healing begins. Within hours, a blood clot forms around the microscopic ridges of the implant surface, releasing signaling proteins that recruit osteogenic (bone-forming) cells. Over the subsequent 3 to 6 months, these cells deposit new woven bone directly onto the implant's surface micro-topography, which gradually remodels into dense, structured lamellar bone. This biological bond provides secondary stability, locking the implant permanently within the jaw.
Clinical Advantages Over Conventional Prosthetics
When evaluating tooth replacement options, dental implants offer several major clinical benefits compared to traditional fixed partial dentures (bridges) and removable full dentures:
1. Attenuation of Alveolar Bone Resorption
When a natural tooth is extracted, the surrounding alveolar bone loses its primary functional purpose—withstanding mechanical chewing forces. Lacking this regular stimulation, the body begins a natural process of bone resorption, causing the jawbone to recede over time. This structural degradation can compromise adjacent teeth and cause noticeable changes to facial aesthetics, such as hollowing of the cheeks and a shortened lower facial height. Dental implants are the only restorative treatment that replaces the missing root, transferring chewing forces directly back into the bone to stimulate and preserve its volume.
2. Elimination of Adjacent Tooth Alteration
To install a traditional three-unit fixed dental bridge, a clinician must permanently alter the adjacent, often completely healthy teeth on either side of the gap. These teeth (abutments) are shaved down to serve as supportive anchors for the bridge, making them susceptible to future decay, pulpitis (nerve inflammation), and structural fractures. Dental implants are completely self-supporting units that preserve the structural integrity of the adjacent dentition.
3. Restoration of Masticatory Force
Traditional removable dentures rest directly on the delicate mucosal tissues of the gums, relying on surface tension or messy adhesives for retention. As a result, denture wearers experience a substantial drop in masticatory (chewing) efficiency, often reclaiming less than 20% of their natural bite force. Dental implants, being anchored firmly into the jawbone, restore up to 95% of natural chewing capacity, allowing patients to maintain a varied and nutritious diet without restriction.
Taxonomy of Implant Variations and Designs
Implant modalities are tailored to accommodate variations in jaw anatomy, bone density, and the volume of missing teeth. Dentists classify implants based on their surgical placement approach:
Endosteal Implants
The most widely used design in contemporary clinical practice. Endosteal implants are placed directly into the alveolar bone. They are highly effective for patients who possess adequate bone height, width, and density to completely surround the fixture.
Subperiosteal Implants
These are used primarily when a patient exhibits severe alveolar ridge atrophy and wishes to avoid extensive bone grafting procedures. Rather than entering the bone, a subperiosteal implant features a custom-contoured metal framework that sits directly on top of the jawbone, underneath the periosteum (the fibrous tissue covering the bone). The framework distributes chewing forces across a wider skeletal surface area.
Zygomatic Implants
When extensive bone loss occurs in the maxilla, traditional endosteal implants cannot be safely placed without significant risk of sinus perforation or mechanical failure. In these complex cases, lengthened zygomatic implants are utilized. These fixtures bypass the maxillary ridge entirely, angling upward to anchor securely into the dense zygomatic bone (the cheekbone).
Digital Workflows: The Contemporary Surgical Protocol
The integration of digital imaging and computer-aided engineering has turned implant placement into a highly accurate, predictable, and minimally invasive workflow.
Clinical Advantages Over Conventional Prosthetics
When evaluating tooth replacement options, dental implants offer several major clinical benefits compared to traditional fixed partial dentures (bridges) and removable full dentures:
1. Attenuation of Alveolar Bone Resorption
When a natural tooth is extracted, the surrounding alveolar bone loses its primary functional purpose—withstanding mechanical chewing forces. Lacking this regular stimulation, the body begins a natural process of bone resorption, causing the jawbone to recede over time. This structural degradation can compromise adjacent teeth and cause noticeable changes to facial aesthetics, such as hollowing of the cheeks and a shortened lower facial height. Dental implants are the only restorative treatment that replaces the missing root, transferring chewing forces directly back into the bone to stimulate and preserve its volume.
2. Elimination of Adjacent Tooth Alteration
To install a traditional three-unit fixed dental bridge, a clinician must permanently alter the adjacent, often completely healthy teeth on either side of the gap. These teeth (abutments) are shaved down to serve as supportive anchors for the bridge, making them susceptible to future decay, pulpitis (nerve inflammation), and structural fractures. Dental implants are completely self-supporting units that preserve the structural integrity of the adjacent dentition.
3. Restoration of Masticatory Force
Traditional removable dentures rest directly on the delicate mucosal tissues of the gums, relying on surface tension or messy adhesives for retention. As a result, denture wearers experience a substantial drop in masticatory (chewing) efficiency, often reclaiming less than 20% of their natural bite force. Dental implants, being anchored firmly into the jawbone, restore up to 95% of natural chewing capacity, allowing patients to maintain a varied and nutritious diet without restriction.
Taxonomy of Implant Variations and Designs
Implant modalities are tailored to accommodate variations in jaw anatomy, bone density, and the volume of missing teeth. Dentists classify implants based on their surgical placement approach:
Endosteal Implants
The most widely used design in contemporary clinical practice. Endosteal implants are placed directly into the alveolar bone. They are highly effective for patients who possess adequate bone height, width, and density to completely surround the fixture.
Subperiosteal Implants
These are used primarily when a patient exhibits severe alveolar ridge atrophy and wishes to avoid extensive bone grafting procedures. Rather than entering the bone, a subperiosteal implant features a custom-contoured metal framework that sits directly on top of the jawbone, underneath the periosteum (the fibrous tissue covering the bone). The framework distributes chewing forces across a wider skeletal surface area.
Zygomatic Implants
When extensive bone loss occurs in the maxilla, traditional endosteal implants cannot be safely placed without significant risk of sinus perforation or mechanical failure. In these complex cases, lengthened zygomatic implants are utilized. These fixtures bypass the maxillary ridge entirely, angling upward to anchor securely into the dense zygomatic bone (the cheekbone).
Digital Workflows: The Contemporary Surgical Protocol
The implant teeth price in malaysia of digital imaging and computer-aided engineering has turned implant placement into a highly accurate, predictable, and minimally invasive workflow.
https://www.tidental.com.m...
The field of restorative dentistry has undergone a radical transformation over the past several decades. For generations, individuals suffering from tooth loss were limited to superficial surface-level prosthetics like removable dentures or fixed dental bridges. While these traditional modalities offered basic cosmetic concealment, they frequently failed to stop long-term biological deterioration and presented significant functional limitations.
https://www.tidental.com.m...
Today, dental implants represent the undisputed gold standard for tooth replacement in modern clinical practice. By serving as biocompatible, structural anchors that integrate directly with the human facial skeleton, implants closely match the biological efficiency, tactile sensation, and functional bite force of natural dentition.
For patients managing single-tooth gaps due to trauma, multiple missing segments from progressive decay, or complete edentulism (total tooth loss), dental implants provide a reliable, predictable option for comprehensive oral rehabilitation. This comprehensive clinical article covers the structural engineering, biological mechanisms, diagnostic protocols, and contemporary workflows defining modern dental implantology.
Anatomy and Structural Engineering of an Implant System
A dental implant is not a singular prosthetic component, but rather an assembly of micro-engineered parts that function as a unified structural system. The long-term success of an implant relies on the mechanical connections between three key elements:
The Implant Fixture (Post): This is the screw-like cylinder that is surgically inserted deep into the cortical and cancellous bone of the maxilla (upper jaw) or mandible (lower jaw). It acts as an artificial root. Modern fixtures are heavily engineered using bio-inert materials—most commonly grade 4 or grade 5 titanium alloys, or highly resilient zirconia ceramics. The surface texture is often modified via sandblasting, large-grit acid-etching, or hydrophilic coatings to maximize surface area and accelerate initial cellular attachment.
The Abutment: This is a precision-machined intermediate connector piece that attaches directly into the internal chamber of the implant fixture via an internal hex or conical connection. The abutment transitions the implant system from an intraosseous (inside the bone) anchor to a transmucosal (through the gum tissue) platform, serving as the solid core onto which the visible prosthesis is anchored.
The Prosthetic Restoration: The definitive aesthetic and functional component of the system. Depending on the patient's structural needs, this may consist of a single custom crown, a multi-unit fixed bridge, or a full-arch overdenture. These are typically fabricated from advanced ceramics, lithium disilicate, or monolithic zirconia blocks using computer-aided manufacturing to match natural teeth.
The Biology of Osseointegration
The scientific foundation of modern implantology relies on the biological phenomenon of osseointegration. Discovered by Swedish orthopedic surgeon Dr. Per-Ingvar Brånemark, osseointegration is defined as the direct, rigid structural and functional connection between living bone tissue and the surface of a load-bearing artificial implant, without any intervening soft tissue layers.
When a titanium or zirconia fixture is surgically advanced into a prepared osteotomy (bone site), it achieves immediate mechanical stability known as primary stability. This initial mechanical lock depends entirely on the physical threads of the screw compressing the surrounding bone.
Following placement, a complex cascade of cellular wound healing begins. Within hours, a blood clot forms around the microscopic ridges of the implant surface, releasing signaling proteins that recruit osteogenic (bone-forming) cells. Over the subsequent 3 to 6 months, these cells deposit new woven bone directly onto the implant's surface micro-topography, which gradually remodels into dense, structured lamellar bone. This biological bond provides secondary stability, locking the implant permanently within the jaw.
Clinical Advantages Over Conventional Prosthetics
When evaluating tooth replacement options, dental implants offer several major clinical benefits compared to traditional fixed partial dentures (bridges) and removable full dentures:
1. Attenuation of Alveolar Bone Resorption
When a natural tooth is extracted, the surrounding alveolar bone loses its primary functional purpose—withstanding mechanical chewing forces. Lacking this regular stimulation, the body begins a natural process of bone resorption, causing the jawbone to recede over time. This structural degradation can compromise adjacent teeth and cause noticeable changes to facial aesthetics, such as hollowing of the cheeks and a shortened lower facial height. Dental implants are the only restorative treatment that replaces the missing root, transferring chewing forces directly back into the bone to stimulate and preserve its volume.
2. Elimination of Adjacent Tooth Alteration
To install a traditional three-unit fixed dental bridge, a clinician must permanently alter the adjacent, often completely healthy teeth on either side of the gap. These teeth (abutments) are shaved down to serve as supportive anchors for the bridge, making them susceptible to future decay, pulpitis (nerve inflammation), and structural fractures. Dental implants are completely self-supporting units that preserve the structural integrity of the adjacent dentition.
3. Restoration of Masticatory Force
Traditional removable dentures rest directly on the delicate mucosal tissues of the gums, relying on surface tension or messy adhesives for retention. As a result, denture wearers experience a substantial drop in masticatory (chewing) efficiency, often reclaiming less than 20% of their natural bite force. Dental implants, being anchored firmly into the jawbone, restore up to 95% of natural chewing capacity, allowing patients to maintain a varied and nutritious diet without restriction.
Taxonomy of Implant Variations and Designs
Implant modalities are tailored to accommodate variations in jaw anatomy, bone density, and the volume of missing teeth. Dentists classify implants based on their surgical placement approach:
Endosteal Implants
The most widely used design in contemporary clinical practice. Endosteal implants are placed directly into the alveolar bone. They are highly effective for patients who possess adequate bone height, width, and density to completely surround the fixture.
Subperiosteal Implants
These are used primarily when a patient exhibits severe alveolar ridge atrophy and wishes to avoid extensive bone grafting procedures. Rather than entering the bone, a subperiosteal implant features a custom-contoured metal framework that sits directly on top of the jawbone, underneath the periosteum (the fibrous tissue covering the bone). The framework distributes chewing forces across a wider skeletal surface area.
Zygomatic Implants
When extensive bone loss occurs in the maxilla, traditional endosteal implants cannot be safely placed without significant risk of sinus perforation or mechanical failure. In these complex cases, lengthened zygomatic implants are utilized. These fixtures bypass the maxillary ridge entirely, angling upward to anchor securely into the dense zygomatic bone (the cheekbone).
Digital Workflows: The Contemporary Surgical Protocol
The integration of digital imaging and computer-aided engineering has turned implant placement into a highly accurate, predictable, and minimally invasive workflow.
Clinical Advantages Over Conventional Prosthetics
When evaluating tooth replacement options, dental implants offer several major clinical benefits compared to traditional fixed partial dentures (bridges) and removable full dentures:
1. Attenuation of Alveolar Bone Resorption
When a natural tooth is extracted, the surrounding alveolar bone loses its primary functional purpose—withstanding mechanical chewing forces. Lacking this regular stimulation, the body begins a natural process of bone resorption, causing the jawbone to recede over time. This structural degradation can compromise adjacent teeth and cause noticeable changes to facial aesthetics, such as hollowing of the cheeks and a shortened lower facial height. Dental implants are the only restorative treatment that replaces the missing root, transferring chewing forces directly back into the bone to stimulate and preserve its volume.
2. Elimination of Adjacent Tooth Alteration
To install a traditional three-unit fixed dental bridge, a clinician must permanently alter the adjacent, often completely healthy teeth on either side of the gap. These teeth (abutments) are shaved down to serve as supportive anchors for the bridge, making them susceptible to future decay, pulpitis (nerve inflammation), and structural fractures. Dental implants are completely self-supporting units that preserve the structural integrity of the adjacent dentition.
3. Restoration of Masticatory Force
Traditional removable dentures rest directly on the delicate mucosal tissues of the gums, relying on surface tension or messy adhesives for retention. As a result, denture wearers experience a substantial drop in masticatory (chewing) efficiency, often reclaiming less than 20% of their natural bite force. Dental implants, being anchored firmly into the jawbone, restore up to 95% of natural chewing capacity, allowing patients to maintain a varied and nutritious diet without restriction.
Taxonomy of Implant Variations and Designs
Implant modalities are tailored to accommodate variations in jaw anatomy, bone density, and the volume of missing teeth. Dentists classify implants based on their surgical placement approach:
Endosteal Implants
The most widely used design in contemporary clinical practice. Endosteal implants are placed directly into the alveolar bone. They are highly effective for patients who possess adequate bone height, width, and density to completely surround the fixture.
Subperiosteal Implants
These are used primarily when a patient exhibits severe alveolar ridge atrophy and wishes to avoid extensive bone grafting procedures. Rather than entering the bone, a subperiosteal implant features a custom-contoured metal framework that sits directly on top of the jawbone, underneath the periosteum (the fibrous tissue covering the bone). The framework distributes chewing forces across a wider skeletal surface area.
Zygomatic Implants
When extensive bone loss occurs in the maxilla, traditional endosteal implants cannot be safely placed without significant risk of sinus perforation or mechanical failure. In these complex cases, lengthened zygomatic implants are utilized. These fixtures bypass the maxillary ridge entirely, angling upward to anchor securely into the dense zygomatic bone (the cheekbone).
Digital Workflows: The Contemporary Surgical Protocol
The implant teeth price in malaysia of digital imaging and computer-aided engineering has turned implant placement into a highly accurate, predictable, and minimally invasive workflow.
https://www.tidental.com.m...
Dental Implants Cost | Implant Teeth Price in Malaysia
Dental implants are offered by TI Dental in Malaysia for the most affordable price. Get low cost painless teeth implants treatments in Selangor
https://www.tidental.com.my/malaysia/teeth/dental-implants-cost/
02:37 AM - Jun 24, 2026
Only people mentioned by abinaya545 in this post can reply